I was asked to do a short session at Paediatric Emergencies 2015 (14th October) on the top ten papers over the last 2 years (seems like it was the week for this type of review!).
It was an interesting challenge to define ‘top’ and I took a pragmatic approach of reviewing pemdatabase.org and then checking my long list against the most cited articles on web of science (using pediatric* OR paediatric* AND emergenc* in the MESH and topic headings).
The top 10 were chosen on the basis of interest and future potential to change practice. I’m happy to be challenged and more than willing to accept further suggestions 🙂
(pleaseclick on the box itself to go to the abstracts and the link below it for my thoughts on the paper and reasons for inclusion)
This was a neat study showing the challenge of sepsis recognition in children. Of 6122 children meeting SIRS vital sign criteria (which didn’t include the White Cell Count component which is an obvious limitation.) 81.6% were discharged from the ED not to return within 72 hours. Conversely there were 72 patients who ended up on Intensive Care who didn’t meet SIRS criteria on presentation.
There is an increasing body of evidence supporting the use of ondansetron in children with gastroenteritis. This American study compared the impact of low, medium and high ondansetron use over a 9 year period. Return rates reduced but the use of iv rehydration did not change. While the Northern Americans have a lower threshold for intravenous rehydration than the UK this study is food for thought. I included it because it contained a huge number of patients (804000) and revealed only 13% of children who received iv therapy had actually been given ondansetron. There are dangers in big data analysis but is this unexpected finding simply highlighting poor clinical judgement or suggestive of some other influences and biases on clinical practice in the management of gastroenteritis ?
I recently blogged on this paper which I think will be a game-changer in the future. 300 infants were randomised to either a normal oxygen saturation monitor or one which over read by 4% (i.e a child with 90% saturations would be displayed as having 94%). The primary outcome was normalisation of cough which was similar in both groups but surprisingly infants who received lower total contact with oxygen (the intervention group) had better outcomes and resumed normal feeding quicker than the control group. While the study was not powered to demonstrate these differences I sense a number of similar studies designed to investigate these findings
Great little paper from the PERUKI group demonstrating some significant differences in practice between clinicians in the management of asthma. I picked this paper as we don’t investigate practice variation enough and also because it highlights an overlooked issue in paediatric respiratory pharmacology. Infusions of intravenous salbutamol are weight based and often can result in overall infusions at much higher doses than adults. Variation in practice is relevant as there is a huge difference in a bolus of 5ug/kg and 5ug/kg/min over 1 hour. This study should make every unit consider there iv infusion policy for paediatric asthma.
Lyttle et al. Variation in treatment of childhood wheeze Arch Dis Child 2015 100(2) 121-5
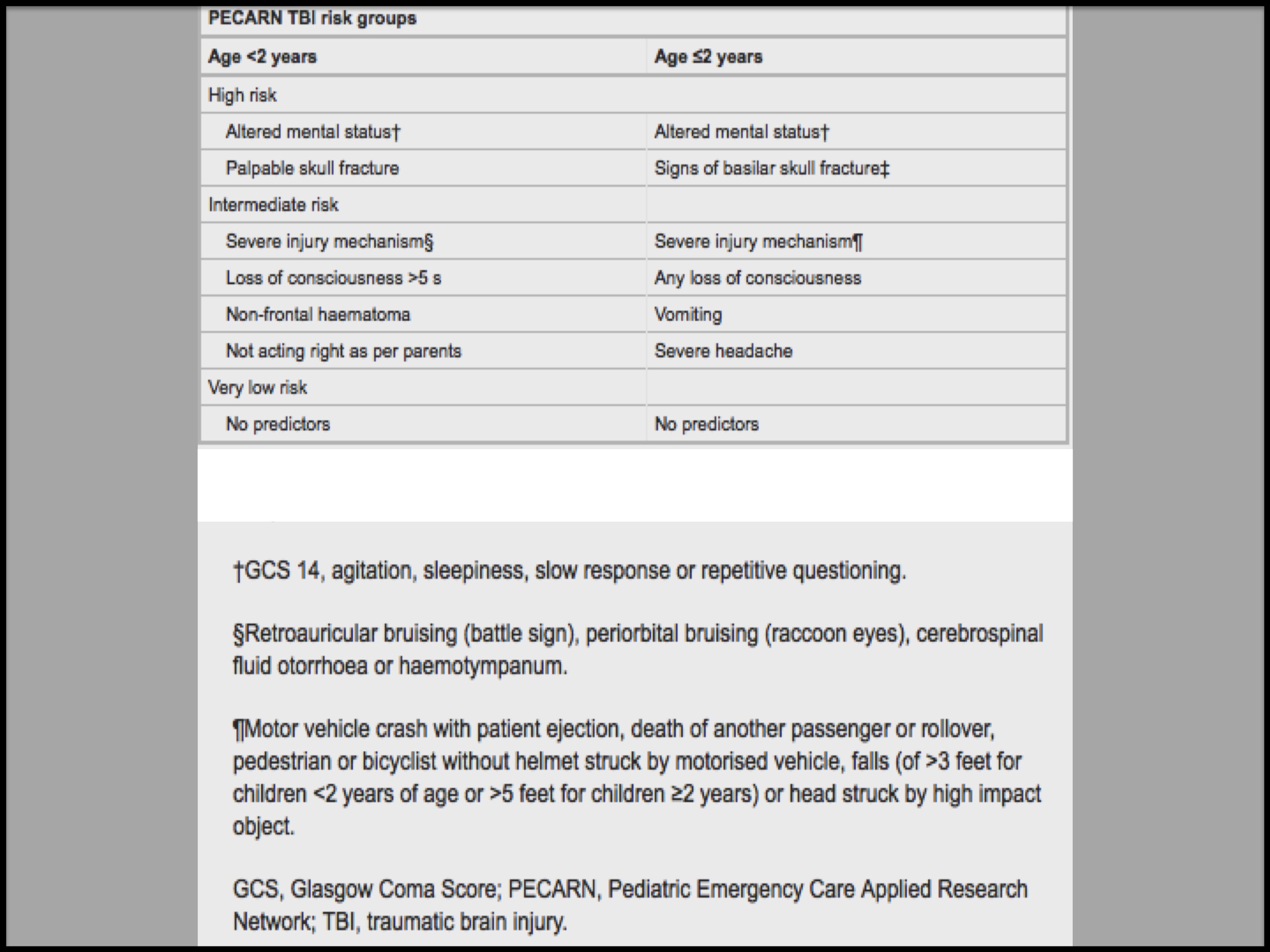
As the quest for the perfect Head Injury Guidance continues the PECARN TBI risk generator (which I think is a good stratification concept in itself) demonstrated good external validity and none of the children with a clinically important TBI were classified as very low risk.
A review of 159 tibial fractures in children under the age of 12. 9% were open injuries and 1/3 needed an operative intervention. None developed acute compartment syndrome. Not a ground breaking paper you may think but how much dogma is there on observations and management based on presumed risk rather than good clinical judgement and safety netting. A call to arms for any unit that just ‘admits for overnight observation’.
The untimely death of John Hinds I suspect will lead to a increased awareness of the risks and benefits of resuscitative thoracotomy. This 20 year series and systematic review found no reported survivors of blunt trauma under the age of 14 years. The figure below (click to enlarge) is stark but a reminder of the destructive influence trauma can have.
Increasing use of electronic patient records will enable to us continually refine and develop algorithms, perhaps in realtime, based on observations and investigations which will benefit and optimise patient outcomes. O’leary et al’s study of over 110000 heart and respiratory rates should make use question the continued use of the defined APLS cut-offs. However, until electronic interfaces are universal in health care it seems likely the pragmatic and very easy to follow APLS guidance will be with us for some time yet.
As a quick aside the paper also drew attention an under-recognised problem of terminal digit preference. How many observations are a reflection of the patients true physiology..?
From O’leary et al. Defining normal ranges and centiles.. Arch Dis Child 2015 100(8) 733-7
So I confess to a certain amount of bias in this area! This is a relevant study for any Emergency Department having a PEWS thrust upon them. While they may be useful at identifying the most critically unwell patients (which Emergency Departments probably don’t do too badly at to begin with) they aren’t so good at recognising need for admission. The area under the ROC curves for predicting hospitalization was poor to moderate (range: 0.56 [95% CI: 0.55-0.58] to 0.68 [95% CI: 0.66-0.69]) across 10 different PEWS
Any intervention that may improve outcome from out of hospital cardiac arrest is welcome. Sadly therapeutic hypothermia had no better functional outcomes for children a year post arrest than current standard care.














{kind=link}
{kind=link}
{kind=link}

