I'm a Consultant at the University of Leicester NHS Trust and Honorary Professor at the University of Leicester. I specialise in Paediatric Emergency Medicine and am a passionate believer that education exists to be shared – the #FOAMed social movement providing a mechanism to do this.
Winter pressures are right on top of emergency and urgent care services at present with hospitals and community practices throughout the UK experiencing high demand and high acuity in a system that is already working at capacity. Clearly maintaining patient safety in this stressed system is vitally important. I chanced upon an interesting view point from Charles Vincent in a Health Foundation blog this week:
“Very few safety strategies are aimed at managing risk in the often complex and adverse daily working conditions of health care”
He argues that current strategies are often designed in ideal environments working in optimum conditions and explores the need to identify and respond to risk in the ‘real world’.
This struck a chord as often health care providers develop specific escalation polices for adverse times only during, or after, these events have taken place. This, on reflection, is a little binary. The ‘real’ world isn’t split between normal practice vs extreme events. While we might aim to grade our response to avoid this dichotomy (in terms of when to contact seniors, where to re-direct flow and who to move into different areas etc.) the ‘real’ world is a variable and dynamic place.
Furthermore Vincent argued that sometimes the actions clinicians and managers take to avoid risk are not always seen under the umbrella of patient safety (and vice-versa). To explore some of the differences the Health Foundation have created a checklist for safety solutions. While it is not immediately obvious how some of the points are directly applicable to a winter crisis the checklist is food for thought in looking at risk and improving safety in any situation.
via the Health Foundation http://www.health.org.uk/sites/default/files/SafetyChecklist.pdf
The financial challenge facing the National Health Service is huge. In the first quarter of this year it overspent by £1.62 billion. This is a difficult figure to comprehend so here is a comparator by John Appleby of the King’s Fund
“Alternatively, the NHS could have saved £1.62 billion by not paying NHS consultants for 5 months; or registrars for 10 months; or nurses for 2 months; or senior managers for 26 months…”
Even the additional funding in the recent spending review is only going to steady the ship for a short period; leading many to question will it ever possible to balance the books? While delivering economic stability may not be felt to be within the remit of health care professionals we must have some responsibility. But how?
This week Roy Lilley and colleagues celebrated the inaugural Academy of Fabulous NHS Stuff awards [1]. The event celebrated the sharing of practical innovation and effective healthcare delivery. The underlying tenet was very similar to that of NHS Change Day. How can we share and learn from what we already do rather than spend more money only to repeat mistakes or unnecessarily create a bespoke ‘local’ version? Joe McCrea had initially introduced me to the idea of capturing the NHS’s social capital. This is not easily defined but to me is the value ascribed to the knowledge that already exists within staff and organisations. It is not always financially tangible but the ‘product’ should be able to be described. Examples of this are the paired learning initiative of bringing together junior doctors and managers or the “pre-loved” idea from Milton Keynes whereby furniture is actively re-distributed around the trust rather than being thrown away.
The Academy of Fabulous NHS stuff website and Change Day stories are a great example of the sharing of social capital. However their impact is only as good as the relevance of the information to others on those sites. The opportunities to use the social capital of the NHS are everywhere however. From a simple handover of the overnight take to a more formal review of a service we are, to some extent, utilising the knowledge and skills of our staff. Choosing to listen to what is being said, and responding and replicating to initiatives and ideas that work, may well be the way that all staff can contribute to financial challenges ahead.
What have you learnt this week? #WILTW
[1] Award ceremonies are a polarising phenomenon. Many believe the celebration of achievement is an important moral boost and creates a positive culture while others think the cost involved is not balanced by any tangible gain. To mitigate this the event was held at no cost to the participants and had a focus on pragmatic revelery rather than traditional ‘three-course’ dining but ultimately the cost of the event was balanced by obvious sponsorship. My gut feeling is the benefit of the event outweighs the counter-concerns but appreciate the jury is still out on this.
There are many things that make medicine an immensely rewarding career. It may be the ability to meld scientific endeavour with artistic application, the enjoyment of human interaction or the diversity of challenges that pathology, of any type, brings with it.
Medicine can also be extremely hard. Not just physically but emotionally and often spiritually (whether religous or not). There are periods when, if you let it, it can become all consuming. Some of this might might be self induced, “I must stay late to finish this project or paper” but at other times just a consequence of the pressure and scale at work. Winter can be a tough time with large patient volume, a proportionally higher risk of missing subtle serious illness and often greater patient or family anxiety due to a system stretched to capacity.
Before a busy shift this week I felt a great sense of unease. The joy of medical practice had gone. Replaced by a sense of almost resentment and resignation at the demand of managing a department that would likely be full to capacity. I have previously been proud of my resilience, a concept I first heard about through social media. I was introduced to the flipside of resilience in a fantastic post by Jonathon Tomlinson. It was actually on empathy but a spin out conversation led to a discussion on burnout. If I had not read this I may have put my state of mind down to tiredness. Although it remains perfectly possible that I was simply exhausted the advantage of putting aside the time to write this weekly blog has enabled me to actively sit down and reflect on where I am truly at.
via Life in the Fast Line (http://lifeinthefastlane.com/ccc/burnout/)
Burnout can be a dangerous thing, just as much for your patients and colleagues, as well as yourself. I score highly on burnout scores so I think I would be in denial if I put my feelings down to recent winter pressures. I am also actively aware I can put in place mitigating factors to protect myself. This is one of the most uncomfortable #WILTW I think I have written. Whether I am being brave or stupid I don’t know but in doing so I feel a small weight has been lifted. I can avoid burning out by being aware of its signs and symptoms and am grateful to Andy Bradley in this regard (his great Ted Talk has been instrumental in developing my own mindfulness). In order to respond, you must recognise, a vital first step in a learning process.
Locally and regionally it has been a tough week for Children’s services. We have not only seen our usual seasonal spike in attendences but a far more virulent strain of parainfluenza (a cause of croup) and high demand for high dependancy and intensive care beds.
The hospital has been full to capacity and this creates a situation where all areas are working flat out to ensure patients are safe and being managed as effeciently as possible. In some respects for those working in emergency and acute care this is ‘our moment‘. At times of crisis we have a body of staff who are trained to manage the most challenging circumstances with professionalism and diligence. While it may be testing, and certainly exhausting, there is an inherent reward in the feeling of a job well done. At some level it must also be enjoyable, even if not constantly so, as otherwise it would certainly not be sustainable. A degree of pressure releases adrenaline which serves, for short periods, as a drug to get you through the most difficult periods.
I muse on this as I recently picked someone up on social media for describing the performance of a critical intervention on a child as ‘exciting’. This made me feel uncomfortable. I am 100% sure the person was not being gung-ho as the comment was acutally made in comparison to the anticipation felt about a forthcoming event. But while I too have heightened awareness when life saving procedures are needed I am not sure I am excited by it. I have previously described my narcicissm when it comes to emergency care and the positive nature of the teams of people I work with. I would hope though that the satisfaction derived from performing a technically difficult produre does not interfere with my situal awareness for that patient. This to me is the danger of excitement in clinical medicine. It is a narcotic that could be dangerous. Conversely I recognise the difficulty in semantics and I may simply be over-interpreting a short sequence of words!
What is certain is that at times of greatest demand, people need some return on their emotional and physical investment. I am hugely grateful to all the staff I work with for supporting each other through this difficult time. Emergency and urgent care need to be enjoyable, and perhaps indeed an exciting place to work, as long as that excitement is derived from the passion and adrenaline of the whole environment.
Virtually everyone adopts some form of dental hygiene. Some people employ sleep hygiene and others have to be very aware of their own personal hygiene. I suppose it shouldn’t have been a surprise then when I was asked this week about Social Media Hygiene.
Unlike dental or sleep hygiene there isn’t an clear benefit to Social Media hygiene. You brush your teeth to stop them rotting. What are you aiming to avoid with good Social Media practice? I suppose for me it is avoid having an adverse impact on my work and family life. I use Social Media to filter knowledge and improve my research capacity. This shouldn’t be at the expense of anything else.
I could instantly think of a couple of things I’ve needed to clean up over time but my gut reaction was that I would have a good rating on any external inspection. On reflection however I am not sure this is actually the case.
So what I have learnt to do?
Not say things online I wouldn’t be able to say to someone’s face This is simply good practice.
Not to take views on Social Media (in particular twitter) as representative
There is a temptation to get carried away with trending discussions only to find they are solely held by the type of people who like to spend a lot of time on social media. These views are not necessarily wrong but not everyone may share them.
Not to get upset or angry that others don’t share my views Be frustrated, yes, but some people, even your colleagues, will have different principles that you may venomously disagree with. Social Media brings these out into the open. There is nothing wrong with discussing them but there are some people who you will not change. And remember – they may be thinking the same about you.
What am I aware of but haven’t perfected?
Not blogging or micro-blogging with expectation One of my most painful admissions is the occasional disappointment at a blog or tweet not being as popular as I think it should, or would, be.
Not being jealous This is probably more a personality flaw than a hygienic approach. I’ll confess I have wondered why some things appear to go viral which are either stupid, obvious, evangelical or something I’d already said. I admit to still not completely being able to shake this.
Switching off The CAGE questionnaire is used to assess for potential alcohol problems and asks questions about an individuals drinking.
Have you ever thought of Cutting down? Do you get Angry if someone asks you about it? Do you feel Guilty? Have you ever had an Eye-opener?
Anyone challenged you on how much time you spend on social media? Do you reach for your phone first thing in the morning?
What I’m still bad at
Online conversations are not the same as face-to-face ones I have this silly habit of not wanting to leave a twitter discussion mid-stream or feel I have to comment on someone else’s posting. Is this really ever that urgent? Can I honestly say I haven’t done this at the expense of a conversation with someone I am physically in the same room with?
I can’t. Definitely unhygienic .
I am not sure whether Social Media ‘hygiene’ is a real thing or not but I do know there is much I can still do to improve my use of it.
Trip-advisor and related review websites have revolutionised realtime feedback to organisations. This is not just limited to hotels and restaurants as both Patient Opinion and NHS Choices allow ‘consumers’ to rate the care they have been given in health care settings. However individual feedback is a different matter. Doctors tend to receive anonymised 360 degree feedback. This consists of colleagues (of varying professions) rating a doctors’ performance across a number of domains and being able to provide short comments about them (but not needing to identify themselves). There are mixed views on this approach but it is useful for those who lack insights into certain behaviours to receive feedback in a way that doesn’t promote individual conflict.
This week I put my mouth in gear before engaging my brain at a meeting and said something I hadn’t intended to. It wasn’t something I thought was actually true just a very poorly thought out quip. This wasn’t the first, and won’t be the last time, I do this I am sure. The reaction of my colleagues surprised me though – a number felt it was very out of character for me to make sweeping generalisations and seemed quite taken aback. This is not something I’ve been told before (but at the same time not sure it is something you would actively feed back to someone!) It made me think whether the traditional anonymised feedback process makes it difficult to ascertain what you are normally like, not just what you are specifically good or bad at. You can certainly suggest to people you’d like this feedback but in the context of the way an online 360 appraisal form works this is often not easy to do. Also feedback you feel is important for you maybe different from what is perceived to be relevant by those feeding back. I have often thought health care professionals should undertake the JoHari window exercise more often
JoHari window – via Roland D and Matheson D. New theory from an old technique: the Rolma matrices. Clinical Teacher 2012; 9(3): 143-147The exercise involves a participant selecting, from a list, adjectives which they felt best described their personality. Colleagues of the participant then pick, from the same selection, adjectives which they feel best describe them. Those picked by both participant and colleague represent ‘open’ traits whereas those selected by just the participant would be ‘hidden’. Those selected just by the colleagues are in a more ‘blind’ area and this obviously enables discussion to proceed about interpersonal relationships.
Even just thinking about undertaking a JoHari window makes you wonder about how you will be described. Seeking out open feedback can be quite a challenge so it was interesting to see the success that Anne Cooper had this week in asking for comments on her own digital behaviours. It’s clear the process interested people, as not only was there a great deal of social media discussion about this, the blog has over 45 comments already. I wonder how this process would work for someone who doesn’t have such a large profile as Anne does but it demonstrates such as undertaking is a possibility (although I’m not sure it always needs to be done via social media!)
Anonymised feedback will always serve a purpose but I wonder whether direct “give me what you’ve got” feedback has an important place as well.
The leaves have turned brown, the temperature has dropped and Emergency Departments and wards are beginning to fill with wheezy coughing children. In the Northern hemisphere winter is with us…
Emergency and Urgent Care are often over-burdened by the effects of this seasonal change, which is particularly extreme in children. The predictable increase in respiratory disease this time of year should mean we are experts in its management but the combination of frequent staff turnover and challenging disease phenotypes militates against this.
Why is acute paediatric respiratory disease so challenging?
Different diseases are not only difficult to describe but may co-exist in the same patient
Asthma, Bronchiolitis, Croup and Pneumonia are 4 seemingly distinct clinical entities in children. However there is also this odd condition that exists between bronchiolitis and asthma in the UK termed viral wheeze (or as some family doctors call it: wheezy bronchitis). Finally the most common respiratory ‘condition’ that children acquire is a viral upper respiratory tract infection.
The snotty infant, off feeds with sub-costal recession and a cough, could have any one of these except asthma. Ask a medical student to define asthma and I suspect you’ll get a potentially more correct answer than a doctor in the early years of training. The student may quote the patho-physiological diagnosis of reversible airways disease and bronchial mucus secretion. A clinician-in-training will be honed in on wheeze and prior history i.e. what they see in practice. In the <1 group where bronchiolitis (breathing difficulties, cough, poor feeding in the context of wheeze and/or crepitations on auscultation [1]) is a common differential the diagnostic conundrum versus viral wheeze can cause confusion. Practical definitions are often worthless until you see enough cases to be able to apply pattern recognition.
Croup is technically an easier diagnosis – a pattern of characteristic cough and stridor differentiates it from other respiratory conditions.
However it’s not uncommon to see a child with stridor and a history of barking cough but wheeze on auscultation and a prolonged expiratory phase. There is an association between croup and asthma and certainly a proportion of children can have mixed signs. This isn’t unsurprising as parainfluenza or any of the other viruses that can cause croup can set off the inflammatory cascade that typifies viral wheeze and asthma.
Finally pneumonia is one of those terms which is frequently used in different ways by health care professionals and the public. Lower Respiratory Tract Infections may be bacterial or viral in origin and although pneumonia (an infection or inflammation of the lung caused by nearly any class of organism) can also be either it is often used to imply a bacterial cause. Diagnosis using clinical signs is fraught with challenges (regardless of how clear the crackles are after having seen the x-ray). There is often an (unnecessary) tension to exclude pneumonia as the cause of the severity of a child’s condition in asthma or bronchiolitis. Which leads us nicely onto judgements of illness severity – a real but often unrecognised health system challenge.
Mild, Moderate and Severe Acuity Descriptors have inherent face validity but their assessment is more complex than the clinical features alone.
Both professionals and members of the public would probably have a similar opinion on the severity of respiratory distress in this child
However we know there is large inter-observer variability in assessment. My own work has shown that experienced paediatricians differ in their interpretation of the severity of specific clinical signs.
To be fair, interpretation of respiratory signs was probably the least variable (compared to alertness, hydration status etc.) but 40% of participants still differed in their assessment in this category. There are numerous reasons for this (blog pending on the role of gut instinct in interpretation of clinical signs) but one explanation is that specific features of respiratory distress don’t take into account previous illness trajectory. Typically a clinical feature (moderate recession etc.) will be linked to a degree of severity or a specific score. This is done in isolation of the other clinical features and doesn’t contribute to an overall impression of whether the child may be tiring or not.
How “severe” is the respiratory distress in this 8 month old child?
The child is grunting, has subcostal recession, and a raised respiratory rate (saturations were 94% in air). The underlying diagnosis could be anything from viral wheeze to pneumonia but you’ll have to take my word for it that this little guy had viral wheeze. On a published score relevant to the child’s age he would be at least moderate to severe. In practice an overall impression is also made on how long you think he will be able to sustain that level of work of breathing for. Part of this decision is based on experience and hence the variability of response when I show this video to different clinicians; from “wow, he is sick” to “yes he is working hard but he is not too bad”
Trajectory of illness is important. A child at point x may have been observed to be getting better (A) or getting worse (B). To an external person arriving to review the child there will be no difference between A and B but to the observing clinician their judgment on illness has been altered by how the child’s acuity has changed over time. There is a complicated third arm as well describing the ‘stable’ child who may suddenly improve or deteriorate (C1 or C2). Bronchiolitis, especially in neonates, often has this pattern. An experienced clinician develops a feel for the potential for sudden deterioration (although may not be able to explain why) and hence modulates their judgement on severity accordingly.
Acute Paediatric Respiratory Disease can be challenging
Every winter throws up a different severity of viral antigen producing varying intensities and complexities of respiratory presentations. There is not always a definitive best evidence approach. Considering all possible diagnoses, being aware of trajectory of illness and always listening to the parents will at least ensure you don’t get caught out.
I finish with a video of our grunting child taken 6 minutes after the original footage was taken (he received a single salbutamol nebuliser.) Please note the initial noise is from the child in the next cubicle 🙂
Thank you to the parents of these children who kindly consented to the filming and display of the video on an openly accessible site. Parents were keen other health care professionals should be able to learn from them.
[1] This is taken from the SIGN Bronchiolitis 2006 guidance – although out of date the definition itself I think is pragmatic and remains credible
It is late at night. A doctor in an Emergency Department has just reviewed a nine month old infant. He clicks “discharge” as a final instruction into the hospital’s electronic medical record (EMR) system. An algorithm kicks into life and compares the initial observations of the child with its most recent set. It highlights a persistence of a slight tachycardia for age (calculated against a perpetually updated data set of all the children presenting to the hospital over the last 5 years) despite a lowering of the child’s temperature. A voice analysis device, installed into all cubicles, detects hesitancy and doubt in the mother. Finally it notes a cousin of the child (the EMR matches against all possible genetic records) died secondary to pneumonia when only 6 months old.
This combination of findings prompts an alert. A video of the child (all patients are monitored in real time) is sent directly to the audio-visual doctor arbitrator (ADA) who cancels the discharge and alerts a senior clinician to review the child.
While this may seem Orwellian it is not an inconceivable possibility. Hospitals already have the ability to constantly record patient observation data and some have explored the use of constant video recording. It is possible to undertake sentiment analysis on people’s speech and there is no current reason why third parties (especially if not human) would not be able to match patient records looking for risk factors for immunodeficiency or genetic disease if it would be in a patient’s best interest.
So if we accept the technology is possible when should an ADA be called? In the dying seconds of the Australia vs Scotland Rugby World Cup Quarter Finals Australia were awarded a controversial penalty. The conversion of the penalty resulted in Australia stealing victory from Scotland. Had it been reviewed by the Television Match Official (TMO) it probably would not have been given. However rugby laws did not give the referee the option of seeking TMO assistance in this case. But should all decision be reviewed by a third party? The sporting community would wince at such an infringement of the rapid, spontaneous nature of contact games.
What of medicine when patient safety is stake? Clearly capacity is a obvious obstruction – not all patients can be directly reviewed by someone more senior (although currently certain high risk groups are afforded this in emergency medicine.) So who chooses?
The Doctor – well useful if they are not sure but most mistakes will be unconscious error i.e. you can’t predict when you are going to make a mistake or otherwise you wouldn’t make the mistake….
The Patient – Could lead to a paradigm shift. We know parents may be as good, if not better, than health care professionals at detecting serious deterioration. In Australia there is a system called Ryan’s rule enabling the public to ring a hotline if they think a bad decision has been made about a family member.
A Computer – As in the example there is no reason why algorithm based technology could not be used to identify those patients who have management plans that might go against standard practice (which could be to discharge or admit).
A Watcher – Could there be a permanent virtual referee as an ADA? Observing from a distance and picking patients at random, or perhaps by gestalt and experience, for closer inspection.
So will ADA’s transform medicine or as in the Rugby World Cup just create another mechanism for potential system failure. And do we know what the conditions are for when they should be used? Given that almost anyone would agree a third party opinion is useful when a difficult medical decision has to be made is it now a question of when rather than if?
What have you learnt this week? #WILTW
…entirely randomly during the writing of this piece @natalieblencowe drew my attention to this:
I was asked to do a short session at Paediatric Emergencies 2015 (14th October) on the top ten papers over the last 2 years (seems like it was the week for this type of review!).
It was an interesting challenge to define ‘top’ and I took a pragmatic approach of reviewing pemdatabase.org and then checking my long list against the most cited articles on web of science (using pediatric* OR paediatric* AND emergenc* in the MESH and topic headings).
The top 10 were chosen on the basis of interest and future potential to change practice. I’m happy to be challenged and more than willing to accept further suggestions 🙂
(pleaseclick on the box itself to go to the abstracts and the link below it for my thoughts on the paper and reasons for inclusion)
This was a neat study showing the challenge of sepsis recognition in children. Of 6122 children meeting SIRS vital sign criteria (which didn’t include the White Cell Count component which is an obvious limitation.) 81.6% were discharged from the ED not to return within 72 hours. Conversely there were 72 patients who ended up on Intensive Care who didn’t meet SIRS criteria on presentation.
There is an increasing body of evidence supporting the use of ondansetron in children with gastroenteritis. This American study compared the impact of low, medium and high ondansetron use over a 9 year period. Return rates reduced but the use of iv rehydration did not change. While the Northern Americans have a lower threshold for intravenous rehydration than the UK this study is food for thought. I included it because it contained a huge number of patients (804000) and revealed only 13% of children who received iv therapy had actually been given ondansetron. There are dangers in big data analysis but is this unexpected finding simply highlighting poor clinical judgement or suggestive of some other influences and biases on clinical practice in the management of gastroenteritis ?
I recently blogged on this paper which I think will be a game-changer in the future. 300 infants were randomised to either a normal oxygen saturation monitor or one which over read by 4% (i.e a child with 90% saturations would be displayed as having 94%). The primary outcome was normalisation of cough which was similar in both groups but surprisingly infants who received lower total contact with oxygen (the intervention group) had better outcomes and resumed normal feeding quicker than the control group. While the study was not powered to demonstrate these differences I sense a number of similar studies designed to investigate these findings
Great little paper from the PERUKI group demonstrating some significant differences in practice between clinicians in the management of asthma. I picked this paper as we don’t investigate practice variation enough and also because it highlights an overlooked issue in paediatric respiratory pharmacology. Infusions of intravenous salbutamol are weight based and often can result in overall infusions at much higher doses than adults. Variation in practice is relevant as there is a huge difference in a bolus of 5ug/kg and 5ug/kg/min over 1 hour. This study should make every unit consider there iv infusion policy for paediatric asthma.
Lyttle et al. Variation in treatment of childhood wheeze Arch Dis Child 2015 100(2) 121-5
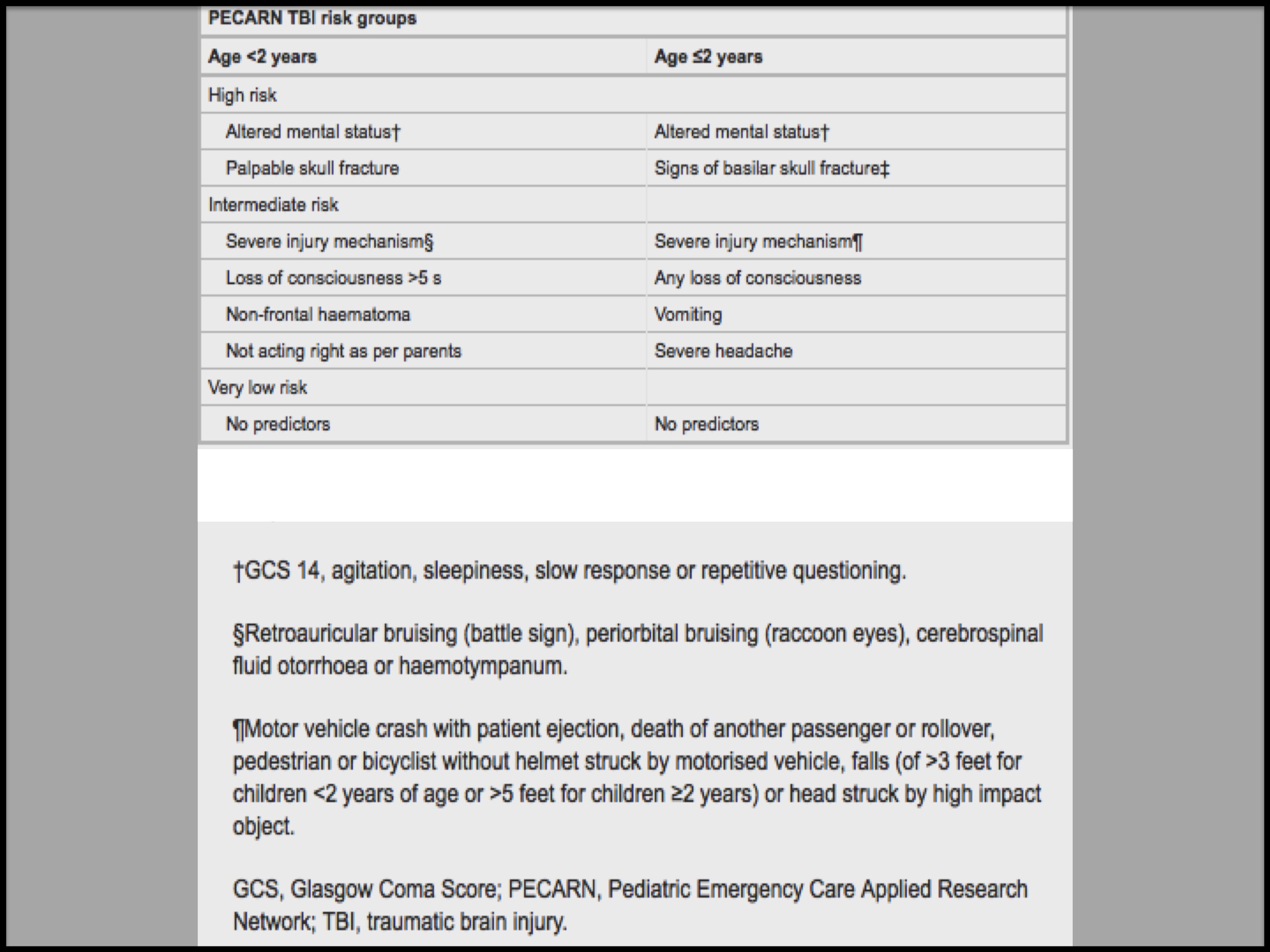
As the quest for the perfect Head Injury Guidance continues the PECARN TBI risk generator (which I think is a good stratification concept in itself) demonstrated good external validity and none of the children with a clinically important TBI were classified as very low risk.
A review of 159 tibial fractures in children under the age of 12. 9% were open injuries and 1/3 needed an operative intervention. None developed acute compartment syndrome. Not a ground breaking paper you may think but how much dogma is there on observations and management based on presumed risk rather than good clinical judgement and safety netting. A call to arms for any unit that just ‘admits for overnight observation’.
The untimely death of John Hinds I suspect will lead to a increased awareness of the risks and benefits of resuscitative thoracotomy. This 20 year series and systematic review found no reported survivors of blunt trauma under the age of 14 years. The figure below (click to enlarge) is stark but a reminder of the destructive influence trauma can have.
Increasing use of electronic patient records will enable to us continually refine and develop algorithms, perhaps in realtime, based on observations and investigations which will benefit and optimise patient outcomes. O’leary et al’s study of over 110000 heart and respiratory rates should make use question the continued use of the defined APLS cut-offs. However, until electronic interfaces are universal in health care it seems likely the pragmatic and very easy to follow APLS guidance will be with us for some time yet.
As a quick aside the paper also drew attention an under-recognised problem of terminal digit preference. How many observations are a reflection of the patients true physiology..?
From O’leary et al. Defining normal ranges and centiles.. Arch Dis Child 2015 100(8) 733-7
So I confess to a certain amount of bias in this area! This is a relevant study for any Emergency Department having a PEWS thrust upon them. While they may be useful at identifying the most critically unwell patients (which Emergency Departments probably don’t do too badly at to begin with) they aren’t so good at recognising need for admission. The area under the ROC curves for predicting hospitalization was poor to moderate (range: 0.56 [95% CI: 0.55-0.58] to 0.68 [95% CI: 0.66-0.69]) across 10 different PEWS
Any intervention that may improve outcome from out of hospital cardiac arrest is welcome. Sadly therapeutic hypothermia had no better functional outcomes for children a year post arrest than current standard care.
“Do you remember that patient you saw last night…?”
Is quite possibly the most terrifying thing anyone can say to a doctor.
The fear is that it’s followed with, “…they have’t done so well” and an implication you have missed something in your investigations or management. It is testament to the generally humble nature of health care professionals that the initial reaction is one of negativity. No one expects, or remembers being told, “Good job!” as the following reprise. Instead there is an expectation of failure or inadequacy.
Simon Judkins is an Emergency Doctor from Australia. This week he published an extract from his book in an newspaper. The short piece was entitled “What did I miss?”. It is powerful narrative in which he is candid about sending home a child at night who returned the next morning with meningococcal septicaemia and needed intensive care treatment. The pain he experienced is obvious from the way he tells the story.
Those who work in acute specialities, especially those in which patients are discharged at all hours of the day, must learn stratagem for dealing with risk. You can not admit and treat all patients who present with a fever. The system would crash and furthermore those most in need of care would no longer receive it. You must make judgement calls. Those who are clearly well or unwell are, generally, easy. But many snotty, slightly miserable children, are brought to Emergency Departments by parents who are concerned about them. Following thorough examination, observation, and investigation (when required), with the important addition of ensuring parental concern has been addressed, many of these children will go home. They are no different to the 11month old Simon Judkins saw.
But you can’t end your shift and worry about all the patients you have sent home. It would not be possible to have a reasonable work-life balance if you did. In fact, I have learnt over time, when I come home uncomfortable about having discharged a child that is a sure sign I shouldn’t have done so. Gut Feeling is a funny thing.
But there is a deeper issue at stake here. I read Simon Judkin’s article and thought – poor guy.
I didn’t think – poor kid.
At least not immediately. It was quite an uncomfortable train of thought. I have written previously about a small aspect of emergency practice that is narcissistic. Not always in a “Look at me!” type way, but a pride in performance, a belief that in some patients you can make a difference. This balances the risks of the job, the possibility that at some stage you will bare the brunt of a poor decision. This I think is an aspect of self preservation. As I become more experienced the total number of patients I see with whom I could make a mistake becomes bigger. I hope the rate of my learning matches the ever increasing level of risk. But I wonder if I have adopted a strategy of risk management that is not primarily aimed at protecting patients but more aimed at protecting me from the ordeal that Simon went through…




























{kind=link}
{kind=link}
{kind=link}